Looking for something?
A Novel Cocktail Drug Penetrates Heart Muscle and May Treat Nearly Half of All Patients with DMD

Duchenne muscular dystrophy (DMD) is a devastating disease that causes the body’s muscle tissues to progressively waste away until all mobility is lost. Eventually, the heart muscle becomes fatty and fibrotic, typically leading to heart failure and death by age 30. There is no cure, and the approved drugs each help a small portion of patients and cannot target the heart muscle. However, a new treatment could help significantly more people with DMD and its associated heart issues.
DMD: a mutation hot spot
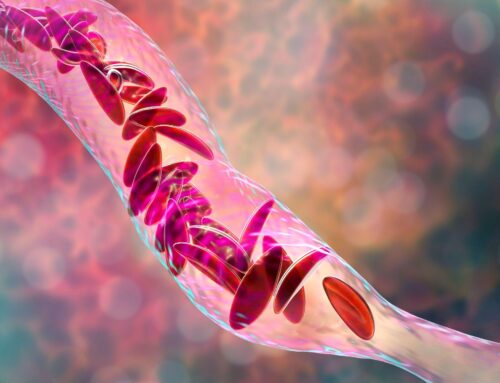
Muscular dystrophy is caused by a mutation in the DMD gene that affects the production of dystrophin, a protein that strengthens, protects, and provides structural support to muscle fibers during regular activities involving muscle contraction and relaxation. Without dystrophin, normal activity causes excessive harm to muscle cells and, over time, the cells are replaced with fat and fibrotic tissue.
The mutation causes muscle damage every time muscles, including those of the diaphragm and heart, contract. DMD causes the body’s muscles to continually waste away until there is a complete loss of mobility and need for a wheelchair often by the age of 12, compromised respiratory and cardiac function by late teens, and probable death by age 30. The disease is more common in males and affects one out of every 3,500 boys and six out of every 100,000 people (1).
Containing 79 connected exons – or sections – DMD is the body’s largest gene, making it highly susceptible to mutations. In fact, more than 7,000 DMD mutations have been identified. Approximately 60-70% of DMD mutations are caused by the deletion of one or more exons that disrupts the protein’s reading frame, resulting in a premature stop codon. If a single exon is missing, the body cannot produce dystrophin and the muscles degenerate.
While there is no cure for DMD, four FDA-approved drugs target specific exon mutations. The drugs are antisense oligonucleotides (ASO) and use phosphorodiamidate morpholino oligomers (PMOs) – synthetic molecules modeled after and containing the same nucleic acid bases as RNA – to skip the mutated exon and link with the next section in the gene. Bypassing the mutated exon repairs the reading frame and creates a shortened but functional dystrophin protein (2).
With only four drugs available, each targeting only one specific exon, the current treatments have limited applicability, and only 8 to 14% of patients benefit (2). However, a team of medical researchers from the University of Alberta has combined six exon-skipping molecules to create a “cocktail” treatment that could benefit far more patients.
New drug: a “cocktail” of benefits
Using peptide-conjugated PMOs, the cocktail drug skips over 11 exons at once, which would allow treatment of up to 47 percent of patients with DMD, explained lead researcher Toshifumi Yokota, a professor of medical genetics in the Faculty of Medicine & Dentistry at the University of Alberta. The multiexon skipping drug (DG9-PMO) bypasses exons 45 to 55, a mutation hotspot in the DMD gene. In addition to skipping multiple exons, Yokota and his team aimed to reduce the number of PMOs needed for the skipping. Using less may improve efficacy, lower the risk of off-target effects, and be more economical (2).
This approach was tested using immortalized patient myotubes – a type of cell that develops into muscle fiber – and DMD mice (H). The results showed that exons 45 to 55 could be skipped by targeting just five exons and that conjugating DG9 – a cell-penetrating peptide – to PMOs improved exon 51 skipping, dystrophin restoration, and muscle function in mice (2).
Results found that DG9-PMO restored an average of 2.5% dystrophin of wild-type levels in mice, significantly higher than that in the saline or PMO groups (2). Compared to the PMO-treated mice, those that received the DG9-PMO had 1.5 to 3.4 higher dystrophin protein levels in skeletal muscles and 4.5-fold higher levels in the heart (2).
“Our cocktail combines the antisense oligonucleotides with a new peptide, a short chain of amino acids, which allows the drug to penetrate the heart muscle,” Yokota said. Targeting the cardiac muscle is a significant advance, as the existing drugs cannot do this, and most patients with DMD ultimately die from heart failure.
Four exon-skipping drugs that have received FDA approval result in an increase of dystrophin in skeletal muscle, but do not target cardiac muscle. Current exon-skipping therapies also have limitations related to PMOs, including their rapid clearance from the bloodstream, reduced uptake into the muscle, and inability to escape from endoscopes (2). A solution to this is the conjugation of cell-penetrating peptides to PMOs, which have widely been documented as improving exon skipping efficiencies and treatment outcomes. DG9 was identified as a promising PMO peptide conjugate (2).
DG9 also has a better toxicity profile than other peptide-conjugated PMOs that have caused dose-dependent symptoms in preclinical studies, including lethargy, weight loss, and kidney damage. The study states that the DG9 peptide was modified, which decreased its antisense activity but improved its viability and safety (2).
“A balance must be struck between efficacy and safety for peptide-conjugated PMOs, as too frequent or too high doses increase toxicity,” the study states, adding that the DG9-PMO caused no liver and kidney damage (2).
Although the DG9-PMO did cause high exon 51 skipping, the dystrophin restoration was generally lower than other peptide-conjugated PMOs. However, the study posits that this may be due to a difference in strategy, as most peptide-conjugated PMO studies perform exon 23 skipping (2).
“Despite its relatively reduced activity, we encouragingly observed functional improvement in mice given repeated doses of DG9-PMO,” the study stated. An improvement in fiber size and an average of 2.8 to 3.9% dystrophin restoration level in the skeletal muscles of DG9-treated mice was observed (2).
“Our finding supports the notion that not much dystrophin may be needed to achieve functional benefit in vivo,” the study said.
The study concludes that future work will focus on evaluating the effects of repeated DG9-PMO therapy on cardiac function and investigating how the efficacy of the minimized multiexon skipping mixture could be increased by varying treatment doses and regimens (2).
“In summary, we have shown proof of concept that a minimized PMO mixture for skipping human DMD exons 45 to 55 could be developed. We have also identified DG9 to be a promising, effective cell-penetrating peptide for PMO conjugation for both single-exon and multiexon skipping approaches,” the study explained (2).
FDA approved exon-skipping therapies
While the cocktail drug must undergo toxicology testing and regulatory steps to conduct clinical trials, four approved exon-skipping drugs are on the market for DMD treatment. Sarepta Therapeutics produces three drugs for DMD treatment, including Exondys 51 (eteplirsen), which is used for the 14% of patients who have a DMD mutation on exon 51, which the drug skips. It was the first exon-skipping drug to receive FDA approval in 2016.
Approximately 10% of DMD patients benefit from the drug Vyondys 53 (golodirsen) and 8% benefit from Amondys 45 (casimersen). Both drugs are produced by Sarepta Therapeutics and are FDA approved. While golodirsen skips exon 53, casimersen works by skipping exon 45.
Viltepso (viltolarsen) is a DMD treatment developed by NS Pharma and based on previous research of Yokota’s. Similar to Golodirsen, the drug treats exon 53 mutations. However, it is four nucleotides shorter than its competition, which may increase dystrophin production. The drug was approved for use in the United States and is currently under review in Canada.
Additionally, in 2021 Sarepta announced the results of the Phase 2 trial of SRP-5051, a second-generation exon-skipping drug that would treat the same patients as Exondys 51. The results suggested it SRP-5051 could offer greater efficacy with less frequent dosing.
Additional progress in multiexon-skipping therapies
Dr. Annemieke Aartsma-Rus, the principal investigator for the DMD Genetic Therapy Group at Leiden University, continues to play an essential role in DMD therapy research (3). Aartsma-Rus’s study used a combination of ASOs to successfully skip multiple exons. The study states that in one patient, exons 43 and 44 were skipped, and dystrophin synthesis was restored. Additionally, the skipping of exons 45 and 51 was achieved in a patient with an exon 46-50 deletion. The study concludes that the in-frame multiexon skipping is a viable option for the various DMD mutations, and it successfully demonstrated the technique’s feasibility (4). Watch this webinar to learn more about selecting ASOs.
The future of DMD treatment
DMD is a devastating and debilitating disease that is difficult to treat due to the various mutation locations. Although there is no cure, current exon-skipping treatments can help ease symptoms. However, these drugs are unable to penetrate the heart muscle, an unfortunate limitation as individuals with DMD often die from heart failure. The new cocktail drug may be an effective solution as results have shown increased dystrophin levels in the cardiac muscle. In addition to improved heart function, the drug has the potential to treat significantly more patients with DMD, offering hope to patients who previously had no options.
References:
- Popplewell LJ, Trollet C, Dickson G, Graham IR. Design of phosphorodiamidate morpholino oligomers (PMOs) for the induction of exon skipping of the human DMD gene. Mol Ther. 2009 Mar;17(3):554-61. doi: 10.1038/mt.2008.287. Epub 2009 Jan 13. PMID: 19142179; PMCID: PMC2835085.
- Lim KRQ, Woo S, Melo D, Huang Y, Dzierlega K, Shah MNA, Aslesh T, Roshmi RR, Echigoya Y, Maruyama R, Moulton HM, Yokota T. Development of DG9 peptide-conjugated single- and multi-exon skipping therapies for the treatment of Duchenne muscular dystrophy. Proc Natl Acad Sci U S A. 2022 Mar 1;119(9):e2112546119. doi: 10.1073/pnas.2112546119. PMID: 35193974; PMCID: PMC8892351.
- Duan, D., Goemans, N., Takeda, S. et al. Duchenne muscular dystrophy. Nat Rev Dis Primers 7, 13 (2021). https://doi.org/10.1038/s41572-021-00248-3
- Aartsma-Rus A, Janson AA, Kaman WE, Bremmer-Bout M, van Ommen GJ, den Dunnen JT, van Deutekom JC. Antisense-induced multiexon skipping for Duchenne muscular dystrophy makes more sense. Am J Hum Genet. 2004 Jan;74(1):83-92. doi: 10.1086/381039. Epub 2003 Dec 16. PMID: 14681829; PMCID: PMC1181915.
Disclaimer:
“The views, opinions, findings, and conclusions or recommendations expressed in these articles and highlights are strictly those of the author(s) and do not necessarily reflect the views of the Oligonucleotide Therapeutics Society (OTS). OTS takes no responsibility for any errors or omissions in, or for the correctness of, the information contained in these articles. The content of these articles is for the sole purpose of being informative. The content is not and should not be used or relied upon as medical, legal, financial, or other advice. Nothing contained on OTS websites or published articles/highlights is intended by OTS or its employees, affiliates, or information providers to be instructional for medical diagnosis or treatment. It should not be used in place of a visit, call, consultation, or the advice of your physician or other qualified health care provider. Always seek the advice of your physician or qualified health care provider promptly if you have any healthcare-related questions. You should never disregard medical advice or delay in seeking it because of something you have read on OTS or an affiliated site.”